Drug Clearance
When administering any medication, it’s crucial to understand how the body handles that drug to ensure it works effectively and safely. Two of the most important pharmacokinetic concepts involved in this are drug clearance (CL) and half-life (t½). These help determine how long a drug stays in the body, how often it should be given, and whether dose adjustments are needed.
What is Drug Clearance (CL)?
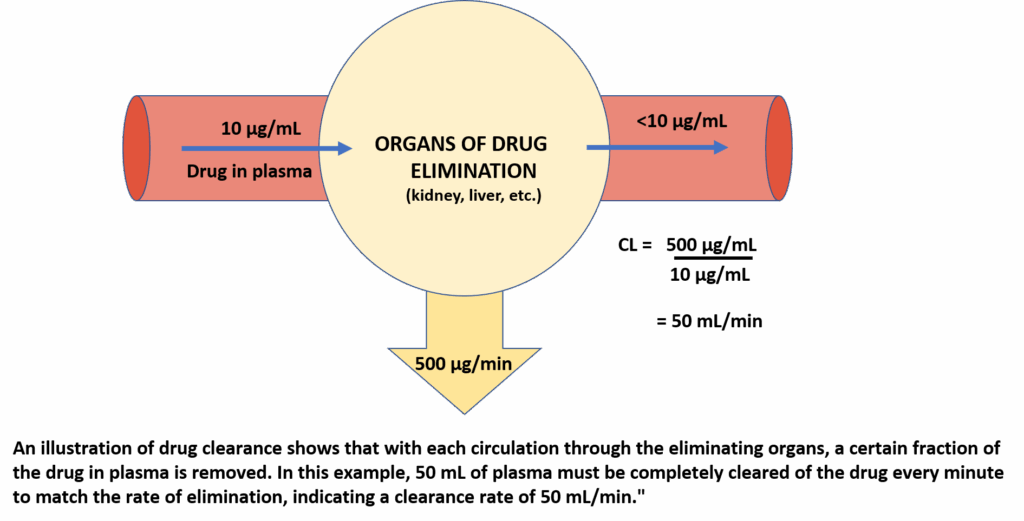
Drug clearance represents the body’s ability to eliminate a drug from the bloodstream. It’s a measure of how efficiently a drug is removed from plasma over time and is expressed in units like mL/min or L/hr.
• Definition: Clearance is the volume of plasma from which the drug is completely cleared per unit time.
• Formula: CL = Rate of Elimination / Plasma Concentration
Types of Drug Elimination Kinetics
Drugs are cleared from the body following two primary kinetic models:
• First-Order Kinetics
– Most drugs follow this model.
– The rate of elimination is proportional to the plasma drug concentration.
– Clearance remains constant.
– Example: Antibiotics, many cardiovascular drugs.
• Zero-Order Kinetics
– Some drugs (e.g., alcohol, phenytoin) follow this model.
– The rate of elimination is constant, regardless of concentration.
– Clearance decreases as the dose increases, making dosing more complex.
• Mixed Kinetics (Michaelis-Menten)
– Some drugs (like phenytoin and theophylline) may exhibit first-order elimination at lower concentrations and switch to zero-order at higher concentrations due to enzyme saturation.
Understanding Half-Life (t½)
Half-life is the time it takes for the concentration of a drug in the blood to reduce by 50%. It gives a practical indication of how long a drug remains active in the system and helps in determining dosing intervals and when steady-state levels are reached.
• Formula (based on elimination rate constant, k): t½ = 0.693 / k
• Formula (in terms of clearance and volume of distribution, V): t½ = 0.693 × V / CL
Half-Life Elimination Timeline:
• After 1 t½ → 50% of the drug is eliminated.
• After 2 t½ → 75% is gone.
• After 3 t½ → 87.5% is gone.
• After 4 t½ → 93.75% is gone.
• After 5 t½ → >95% eliminated.
It typically takes 4–5 half-lives for a drug to be almost completely cleared from the body.
Repeated Dosing and Steady-State Concentration (Cpss)
When a drug is taken repeatedly (e.g., twice a day), it accumulates in the body. Eventually, a steady state is reached, where the rate of drug administration equals the rate of elimination.
• Steady-State Formula: Cpss = Dose Rate / CL
• For oral drugs: Dose Rate = Target Cpss × CL / F (F = bioavailability)
Time to reach steady state: ~4–5 half-lives, regardless of the dose.
Plateau Principle
This principle states that if a drug is given repeatedly at consistent intervals, it will accumulate until a plateau (steady-state) concentration is achieved.
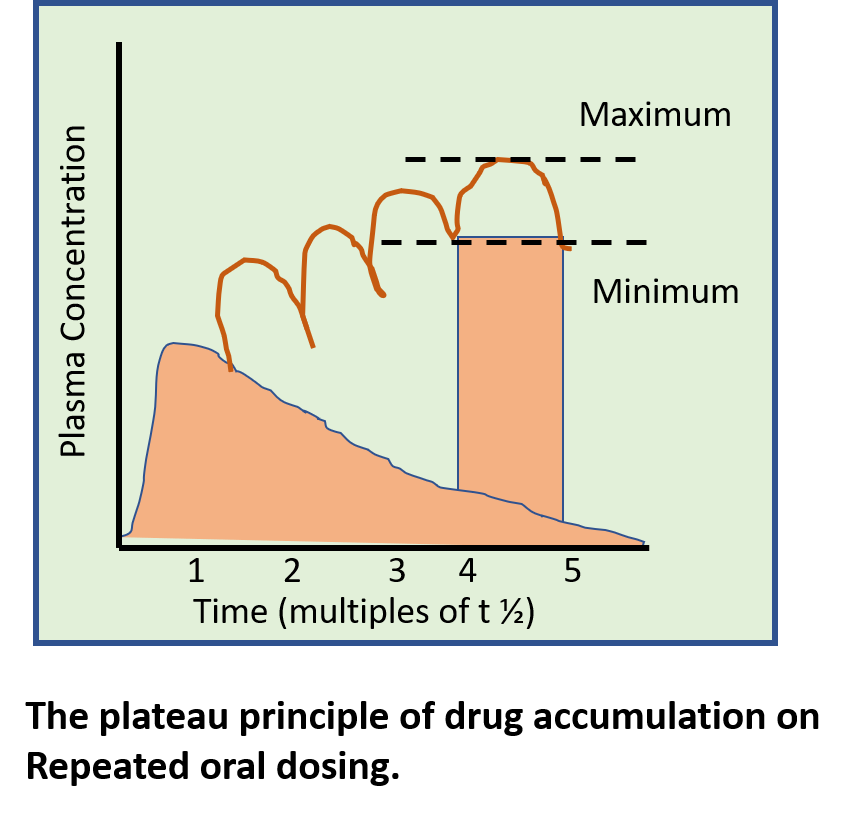
Key insights:
• Dosing before complete elimination causes accumulation.
• Smaller, more frequent doses reduce peak-trough fluctuations.
• Larger, less frequent doses may lead to higher peaks and lower troughs, increasing side effect risks.
Loading and Maintenance Doses
To achieve therapeutic levels quickly, especially for drugs with a long half-life, a loading dose can be used.
Loading Dose:
• A high initial dose to rapidly reach the desired plasma level.
• Formula: Loading Dose = Target Cpss × V / F
Maintenance Dose:
• Smaller, regular doses to maintain plasma drug levels.
• Formula: Maintenance Dose = Cpss × CL
Therapeutic Drug Monitoring (TDM)
TDM involves measuring drug concentrations in blood to optimize therapy—especially important when drugs have a narrow therapeutic index or variable patient responses.
TDM is necessary when:
• Drug has a narrow safety margin (e.g., digoxin, lithium).
• There is large inter-patient variability.
• Organ dysfunction affects metabolism/excretion (e.g., renal/liver failure).
• Checking for compliance or toxicity (e.g., overdose).
When to Sample for TDM:
• Long-acting drugs: Just before next dose (trough level).
• Short-acting drugs: Peak level (1–2 hours after dose).
• Poisoning cases: Immediately, then monitor regularly.
TDM is NOT needed for:
• Drugs with clear, measurable effects (e.g., antihypertensives).
• Prodrugs (e.g., levodopa).
• Irreversible-action drugs (e.g., MAO inhibitors).
Prolonging Drug Action
Extending drug action helps improve compliance, reduce side effects, and simplify dosing schedules.
Benefits of Prolonged Action:
• Less frequent dosing (better compliance).
• Reduced fluctuations in drug levels.
• Maintained therapeutic effect over time.
• Fewer peak-related side effects.
Strategies to Prolong Action:
1. Slow Absorption:
– Oral: Sustained-release tablets or capsules.
– Injectable: Oily depot injections, biodegradable implants, microspheres.
– Transdermal: Skin patches (e.g., fentanyl, nitroglycerin).
2. Plasma Protein Binding:
– Drugs that bind strongly to plasma proteins remain longer in circulation.
– Example: Sulfadoxine.
3. Slow Metabolism:
– Modify drug structure or co-administer enzyme inhibitors.
– Example: Ritonavir boosts levels of other antivirals.
4. Reduced Renal Excretion:
– Compete for renal transporters to slow elimination.
– Example: Probenecid delays penicillin clearance.
5. Targeted Drug Delivery:
– Liposomes: Direct drugs to liver, spleen, or tumors.
– Drug-coated stents and implants: Provide site-specific, long-acting release (e.g., contraceptive IUCDs).
First-Order vs Zero-Order Dosing Caution
• First-order drugs: Safe and predictable. Doubling the dose → double the concentration.
• Zero-order drugs: Dangerous at high doses. Doubling the dose → unpredictable and possibly toxic increase in levels.
Conclusion
Understanding the principles of clearance, half-life, dosing strategies, and therapeutic monitoring is essential for rational and safe drug use. With just a few key formulas and clear concepts:
• Healthcare providers can predict drug behaviour in the body.
• Appropriate loading and maintenance doses can be designed.
• Steady-state levels can be achieved efficiently.
• Monitoring ensures patient safety, especially with critical drugs.
• Prolonged drug action techniques can significantly improve outcomes and adherence. Mastering these pharmacokinetic tools leads to optimised drug therapy, minimised toxicity, and better patient care.
References
Latest Editions of
- Rang H. P., Dale M. M., Ritter J. M., Flower R. J., Rang and Dale’s Pharmacology,.Churchil Livingstone Elsevier
- K.D.Tripathi. Essentials of Medical Pharmacology, JAYPEE Brothers Medical Publishers (P) Ltd, New Delhi.
- Sharma H. L., Sharma K. K., Principles of Pharmacology, Paras medical publisher