Pharmacokinetics: Drug Excretion
The study of how drugs move through the body. Once a drug has been absorbed into the bloodstream and distributed to tissues, the body must eliminate it to avoid accumulation or toxicity. This process of removing systemically absorbed drugs is known as excretion.
Let’s explore how the body excretes drugs through different organs and pathways, with a special focus on the kidneys.
Major Routes of Drug Excretion
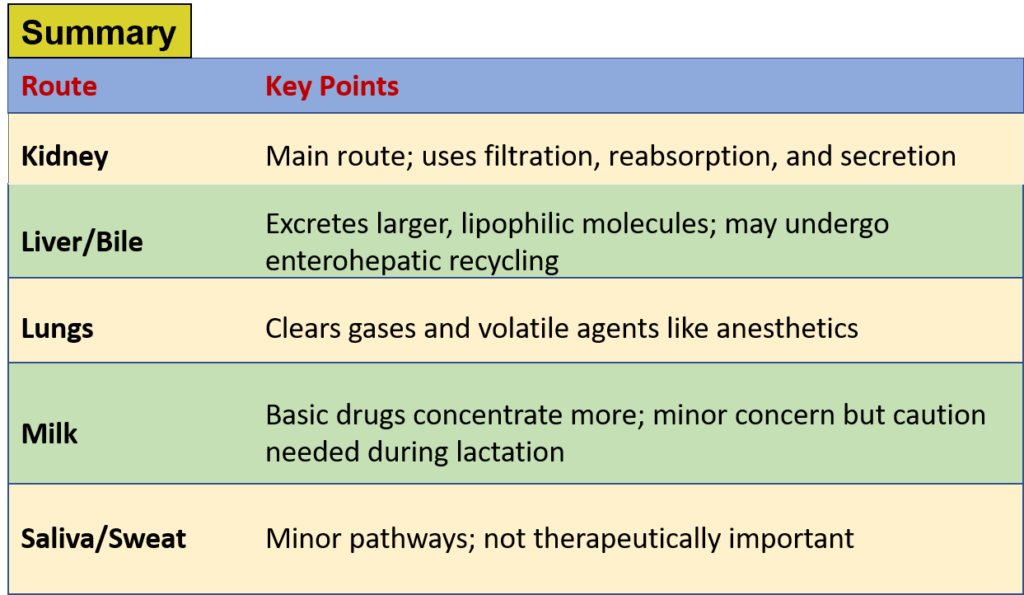
1. Urine (Kidney): The Primary Route
The kidneys are the most important organs for eliminating the majority of drugs. They excrete drugs and their water-soluble metabolites into urine. Renal excretion is especially crucial for drugs that are not metabolized much by the liver.
2. Faeces (Liver and Biliary Excretion)
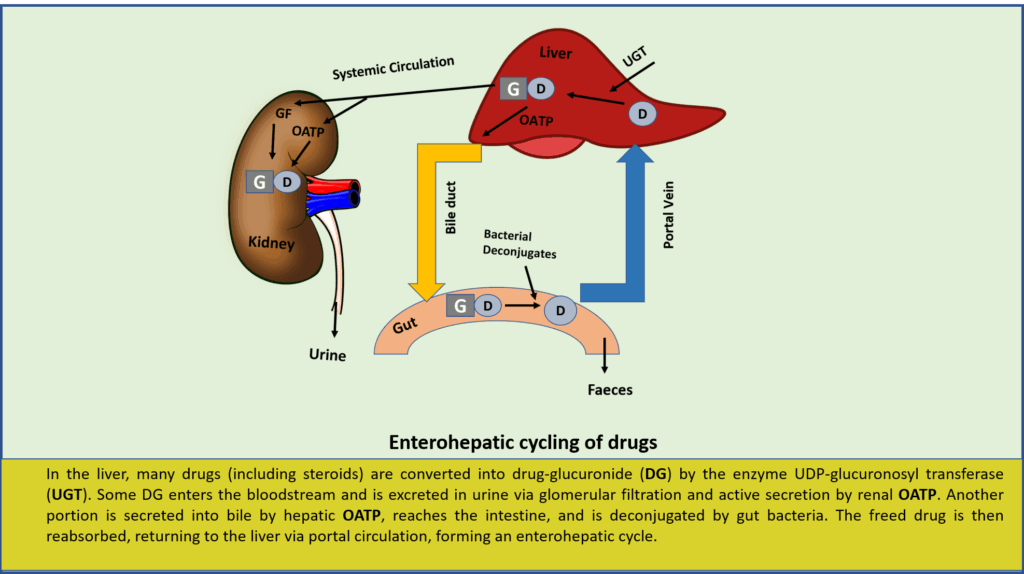
While some drug content in feces is simply unabsorbed drug from the gut, a significant portion comes from the bile. The liver actively secretes certain drugs into bile via specific transport systems:
OATP and MRP2: Transport drug glucuronides (organic acids).
OCT: Moves organic bases.
P-glycoprotein (P-gp): Handles lipophilic drugs.
Drugs with molecular weight greater than 300 are more likely to be excreted in bile. However, many of these are reabsorbed in the intestines through enterohepatic circulation, prolonging their presence in the body.
Examples: Erythromycin, Rifampin, Ampicillin, Oral contraceptives, Tetracyclines
3. Exhaled Air (Lungs)
Volatile substances and gases, such as general anesthetics and alcohol, are eliminated through the lungs. This process is not influenced by lipid solubility but rather by the partial pressure of the compound in the blood.
4. Saliva and Sweat
These are minor excretion routes but may carry small amounts of drugs like Lithium, Iodide, Rifampin, and heavy metals. Although not pharmacologically significant, drugs in saliva are usually swallowed again, re-entering the digestive tract.
5. Milk (Lactation)
Some drugs can pass into breast milk, which may expose nursing infants. Milk is slightly more acidic (pH ~7.0) than plasma, so basic drugs may concentrate more in milk. However, most drugs appear in small amounts, and many are considered safe during breastfeeding. Still, medications should be used cautiously in lactating mothers, only when necessary.
Renal Excretion
The kidneys eliminate water-soluble drugs and metabolites via urine. Three main processes determine how much drug ends up in the urine:
1. Glomerular Filtration
At the glomerulus, only free (unbound) drug molecules are filtered into the renal tubule. The filtration depends on:
- Protein binding
- Renal blood flow and glomerular filtration rate (GFR), normally ~120 mL/min.
GFR decreases with age and in renal disease, reducing drug excretion.
2. Tubular Reabsorption
After filtration, drugs may be reabsorbed from the tubule back into the bloodstream, particularly if they are:
- Lipid-soluble
- Non-ionized at the urinary pH
- Highly ionized or polar drugs (like aminoglycosides) are poorly reabsorbed and are excreted effectively.
Urine pH affects drug excretion:
- Acidic urine increases ionization of weak bases.
- Alkaline urine increases ionization of weak acids.
Used in overdose treatment:
- Alkalising urine for barbiturate or salicylate poisoning.
- Acidifying urine is avoided due to risks like acidosis and toxicity.
After filtration, drugs may be reabsorbed from the tubule back into the bloodstream, particularly if they are:
- Lipid-soluble
- Non-ionized at the urinary pH
Highly ionized or polar drugs (like aminoglycosides) are poorly reabsorbed and are excreted effectively.
3. Tubular Secretion
This is an active transport process in the proximal tubule using specific carriers:
- OAT (Organic Anion Transporters): e.g., penicillin, methotrexate.
- OCT (Organic Cation Transporters): e.g., quinine, cimetidine.
- P-gp and MRP2: Efflux transporters that pump drugs into the tubule lumen.
Even protein-bound drugs can be secreted, making this route crucial for excretion.
Drug Interactions Involving Tubular Secretion
- Probenecid blocks OAT, reducing penicillin excretion and enhancing uric acid excretion.
- Salicylates reduce methotrexate excretion.
- Sulfinpyrazone inhibits tolbutamide secretion.
- Quinidine inhibits P-gp, reducing digoxin excretion.
Drug Excretion in Newborns and Elderly
- In neonates, immature kidneys cause drugs like penicillin to remain longer in the body.
- In the elderly (>75 years), renal clearance declines with age, requiring dosage adjustments.
References
Latest Editions of
- Rang H. P., Dale M. M., Ritter J. M., Flower R. J., Rang and Dale’s Pharmacology,.Churchil Livingstone Elsevier
- K.D.Tripathi. Essentials of Medical Pharmacology, JAYPEE Brothers Medical Publishers (P) Ltd, New Delhi.
- Sharma H. L., Sharma K. K., Principles of Pharmacology, Paras medical publisher